Botulinum toxin injections (Botox® bladder)
What is it?
Intradetrusoral injection of botulinum toxin (Botox®) is a minimally invasive urological treatment designed to reduce the symptoms ofoveractive bladder, such as urgent urges (urgency), frequency (pollakiuria), and emergency bladder leakage when first-line treatments (medication, rehabilitation) are not sufficiently effective.
This treatment involves injecting small doses of toxin into the bladder wall (detrusor), to modulate local nerve activity and reduce involuntary contractions.

In which cases?
Indications
Bladder botulinum toxin injection is considered in the following cases:
- Overactive bladder refractory to or intolerant of first-line treatments (anticholinergics, beta-3 agonists).
- Presence of symptoms including at least:
three episodes of urinary incontinence by urgency over 3 days
– urinary frequency ≥ 8 micturitions per day - Patient acceptance of the risk of transient urinary retention and the possibility ofself-catheterization if necessary.
- Sterile urine at the time of injection (treated urinary tract infection or absence of infection).
Note: in France, Botox’s marketing authorization mainly concerns idiopathic overactive bladder, and its use in this indication must comply with best practice recommendations.
Surgical technique
Here’s how a typical botulinum toxin injection is performed:
1️⃣ Pre-injection preparation
- Cytobacteriological control of urine to ensure absence of infection.
- Urodynamic workup (in many cases) to confirm diagnosis and guide dosage.
- Information, consent, assessment of ability to perform self-catheterization if necessary.
- Local anesthesia (urethral or bladder lidocaine instillation), sometimes sedation or anesthesia depending on the context.
2️⃣ Injections
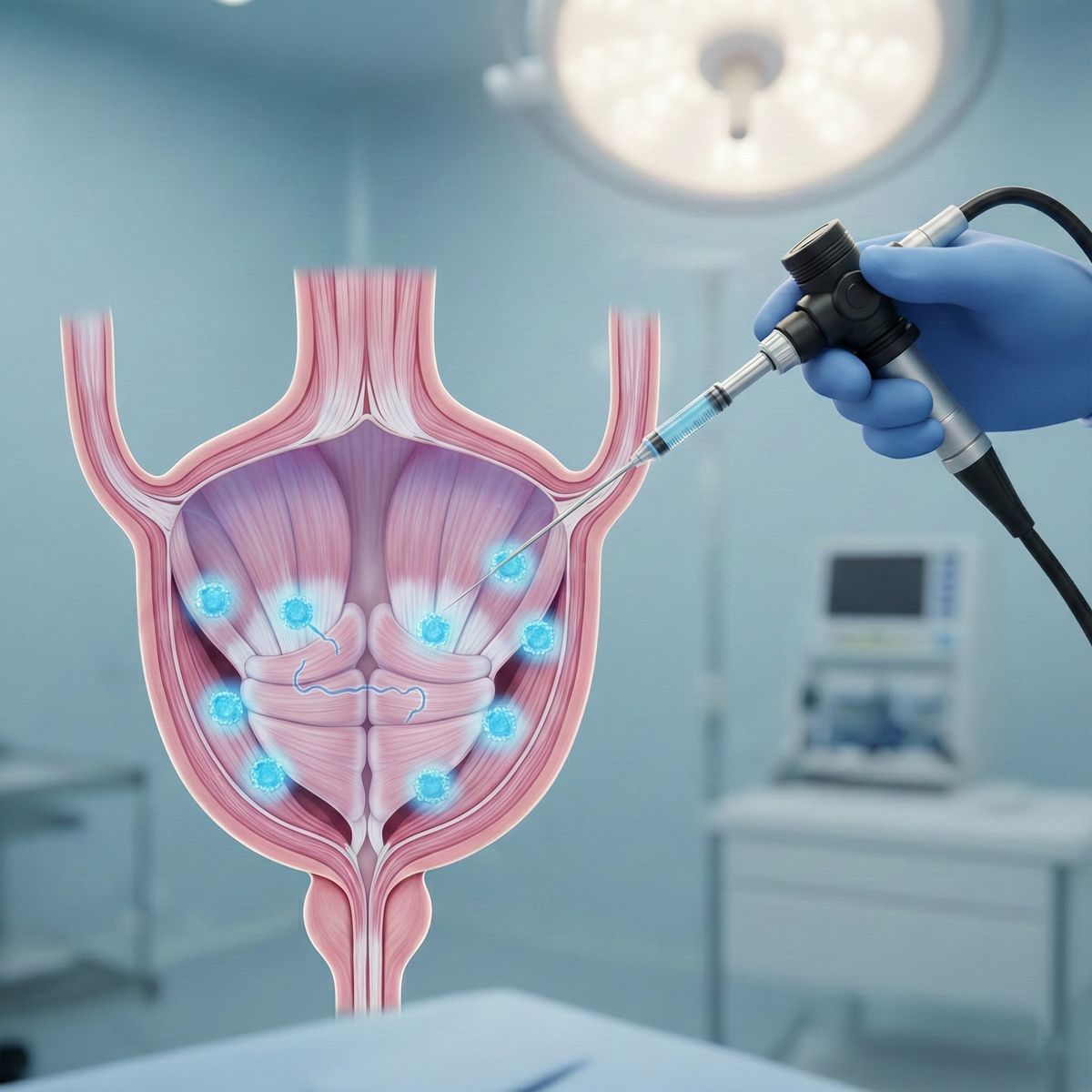
- Endoscopically (cystoscopy): a fine needle injects the toxin into the bladder muscle (detrusor) at 10 to 20 points distributed throughout the bladder wall, avoiding the ureteral meatus.
- Micro-volumes (0.5 to 1 mL per injection, containing several units of toxin) are used to achieve the desired dose.
- Bladder filling is controlled to avoid excessive wall distension.
- It is not necessary to leave a bladder catheter except in cases of severe hematuria.
3️⃣ Duration and hospitalization
What you need to know
Expected results & duration of effect
- The clinical effect generally begins 2 to 10 days after injection.
- On average, the effect lasts 6 to 9 months, depending on the patient and the dose.
- If symptoms return, a further injection may be considered, provided that a minimum interval of 3 months is observed between two injections.
- In studies, Botox use improves urinary incontinence episodes and quality of life, even in patients requiring self-catheterization.
Risks & complications
As with any medical procedure, injecting botulinum toxin into the bladder involves a number of risks:
- Transient acute urinary retention, requiring catheterization or self-catheterization. Retention rates vary according to dose, typically 5-10% in the months following injection.
- Potential urinary tract infection, hence the importance of urine monitoring.
- Temporary hematuria or local bleeding
- Mild to moderate bladder pain or discomfort
- Partial failure or recurrence of symptoms
- Long-term effects still to be monitored (long-term safety profile poorly documented according to HAS).
Contraindications & precautions
- Untreated urinary tract infection
- Hypersensitivity to botulinum toxin
- Neuromuscular pathologies (e.g. myasthenia gravis)
- Anticoagulation not suitable for endoscopic procedures
- Inability to self-flush (in case of retention)
- Pregnancy, breast-feeding (according to medical advice)
- Precautions in the event of an increase in existing post-micturition residue

Botulinum toxin injection specialist
Prof. François Haab is an expert in functional urology, including the treatment of overactive bladder.
✔He performs botulinum toxin injections in compliance with recommendations, with choice of dose and individualized protocol.
✔ It provides rigorous patient support (information, risk assessment, post-operative follow-up).
✔ In the event of reinjection or partial failure, he can suggest complementary alternatives (neuromodulation, drug treatments, etc.).
My journey in video
I made this video to introduce myself and describe my background and expertise.
Make an appointment
I welcome you to my office in Paris to discuss your expectations and propose the most appropriate solution.